PRONE POSITIONING FOR COVID-19 PATIENTS
Prone positioning has been considered for many decades in the management of ARDS. The physiological benefit of the prone position as opposed to the supine include the following:
- Better matching of perfusion to ventilation
- Recruitment of dependent portions of the lung
- Improved arterial oxygenation
- More homogenous distribution of the stresses throughout the lung tissues
The ICU literature has highlighted the importance of EARLY prone positioning in the management of severe ARDS. When patients intubated for ARDS were kept in the
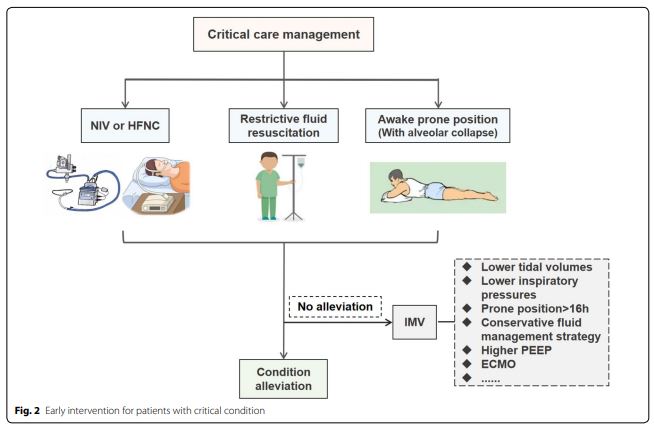
prone position early in their course, their mortality was significantly lower than patients kept in the supine position (Guérin, N Engl J Med). This experience has led to attempts to prone patients in the early stages of COVID-19 acute hypoxemic respiratory failure, long before they might require intubation. The hope was that such an approach would improve their oxygenation and possibly decrease the need for invasive ventilation later on. Physicians in China tried a multi-prong approach that included
proning in a select group of patients (Sun et al. Ann. Intensive Care). Using proning (along with high-flow nasal cannula and restrictive IVF) resulted in only 1% of hospitalized COVID-19 patients needed mechanical ventilation (a truly impressive figure given what has been seen elsewhere).
While proning requires both the patient’s full cooperation (and hence would be difficult in patients with delirium or dementia and in those with restricted mobility) and significant efforts from nursing and respiratory therapy, it can be an effective strategy to rapidly improve oxygenation and possibly decrease the risk that the patient would require intubation.


{kind=link}
{kind=link}
{kind=link}
Wow, thank you for sharing this fascinating study.
Chris
No problem!