In my prior post on estimating surge volume, I reviewed emergency preparedness generally rules of thumb that can be used to estimate volume increases. This is important, of course, since it is critical to understand if there is a ripple or a tsunami coming your way. Ultimately, estimating volume will guide your staffing, determine how quickly you will need recruit others such as primary care physicians to help with inpatient volume, and help you understanding when there may be relief.
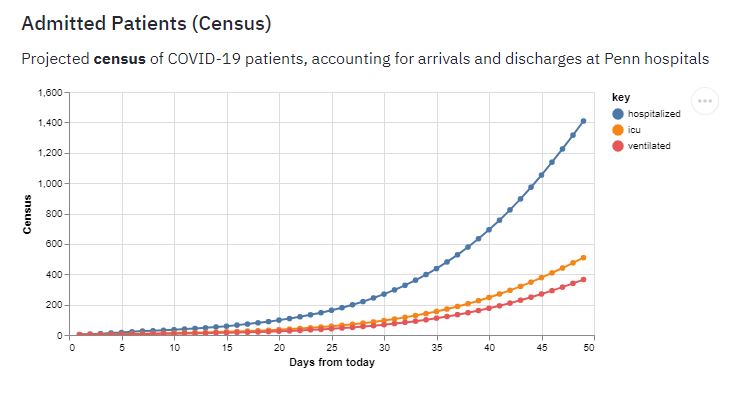
Since that post, a new tool has emerged which I would be remiss if not included here. Penn Medicine’s Predictive Healthcare Team developed a tool called CHIME: The Covid-19 Hospital Impact Model for Epidemics. In this tool, they have already made assumptions about key statistical data which they then applied to a “SIR Model.” I found a very understandable model of what a SIR model is at the Universitat Autònoma de Barcelona at this link. A SIR model enters population data which includes the Susceptible, Infected, and Recovered (SIR) individuals. Several assumptions, including the average number of people any given person will infect, recovery time, and virulence, are plugged into these different populations to yield three quadratic equations which then provide the solution.
As of the date of this post, CHIME just added more instructions on the use. Be sure to follow their directions on the landing page that I provided, or in their more extensive instructions, prior to launching the tool and entering your own data. As they describe on their landing page, modify just the three listed parameters (Currently Known Regional Infections, Currently Hospitalized COVID-19 Patients, and Hospital Market Share). If you are interested in determining how social distancing efforts can “flatten the curve,” you can change the “social distancing” value and see how the curves change.
Thanks to Penn Medicine to helping our hospitalist programs to be better prepared!


{kind=link}
{kind=link}
{kind=link}
Leave A Comment